
Cytomegalovirus (CMV), like EBV, circulates readily among children.
CMV infection is persistent, and is characterised by subclinical cycles of active virus replication and by persistent low-level virus shedding. Most post-childhood infections are therefore acquired from asymptomatic excreters who shed virus in saliva, urine, semen and genital secretions. Sexual transmission and oral spread are common among adults, but infection may also be acquired by women caring for children with asymptomatic infections.
Clinical features Most post-childhood CMV infections are subclinical, although some young adults develop an IM-like syndrome and some have a prolonged influenza-like illness lasting 2 weeks or more. Physical signs resemble those of IM, but in CMV infections hepatomegaly is more common, while lymphadenopathy, splenomegaly, pharyngitis and tonsillitis occur less often. Jaundice is uncommon and usually mild.
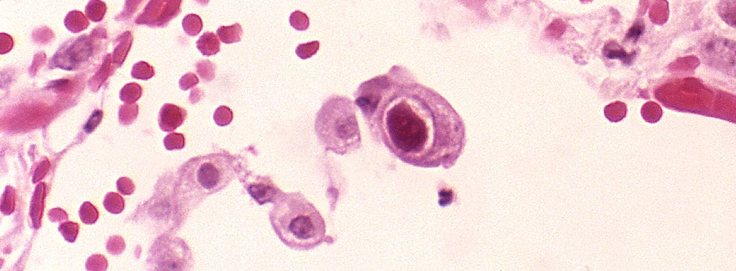
DIAGNOSIS:
COMPLICATIONS include meningoencephalitis, Guillain–Barré syndrome, autoimmune haemolytic anaemia, thrombocytopenia, myocarditis and skin eruptions, such as ampicillin-induced rash. Immunocompromised patients can develop hepatitis, oesophagitis, colitis, pneumonitis, retinitis, encephalitis and polyradiculitis

ABHI HOMEO HALL is a one and half decade old renowned clinic that offers the best quality, non-toxic and highly effective treatment in Ranchi, Patna and Delhi.
Read More

