
ALLOIMMUNIZATION
Alloimunisation (isoimmunization) is defined as a production of immune antibodies in an individual in response to foreign red cell antigen derived from another individual of the same species provided
the first one lacks the antigen. It occurs in two stages
1) Sensitization and
2) Immunization. This is in contrast to ABO groups, where there are naturally occurring isoimmune anti-A and anti-B antibodies.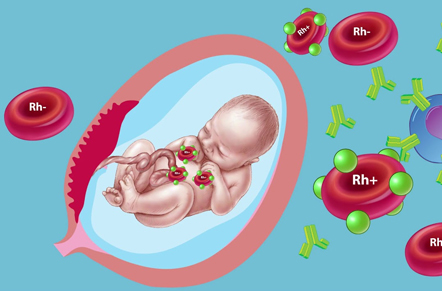
METHODS: -
1) Transfusion of mismatched blood: In ABO group incompatibility, there are naturally occurring anti-A and anti-B isoagglutinins, which result in immediate adverse reaction. In case of Rh group, there is no such naturally occurring antibody and as such there is no immediate reaction but the red cells carrying the Rh antigen sensitize the immunologically competent cells in the body, provided the amount is sufficiently large. This takes at least 1 week. Following a subsequent exposure to the antigen, the cells are stimulated to produce more specific anti-D antibody. The women may suffer a severe hemolytic reaction to the subsequent mismatched transfusion.
2) As a result of pregnancy (Rh-negative woman bearing a Rh-positive fetus). Normally, the fetal red cells containing the Rh antigen rarely enter the maternal circulation. The following are the conditions where the risk chance of fetomaternal bleed is present: miscarriage, MTP, genetic amniocentesis, embryoreduction, ectopic pregnancy hydatidiform mole, CVS cordocentesis placenta previa with bleeding placental abruption, IUFD, external cephalic version, abdominal trauma and the delivery of a Rh-D positive infant to a Rh negative mother. This is much more (15–50%) likely to occur during third stage of labor and following cesarean section or manual removal of placenta. However, recent studies show a continuous fetomaternal bleed occurring throughout normal pregnancies (1%). Immunization is unlikely to occur unless at least 0.1 mL of fetal blood enters the maternal circulation. Not all “at risk” Rh-negative women become alloimmunized. About 17% of Rh-negative women will become alloimmunized by a single Rh-incompatible pregnancy. Rh-sensitization due to antepartum fetomaternal hemorrhage is about 1–2% before delivery. Fetal Rh antigens are present by 38th day after conception. Spontaneous first trimester abortion carries 3–4% risk and that of induced abortion about 5% risk of sensitization. Thus, affection of the baby due to Rh incompatibility is low considering the increased number of Rh-positive babies delivered to Rh-negative mothers.
The reasons are:
- Insufficient placental transfer of fetal antigens or maternal antibodies. -Inborn inability to respond to the Rh antigen stimulus.
- Immunological nonresponder—as found in 30% of Rh-negative women.
-ABO incompatibility has a protective effect against the development of Rh sensitization. This protective effect is significant when the mother is type O and the father is type A, B or AB. The reasons are-
- Variable antigenic stimulus of the D antigen which depends on the Rh genotype of the fetal blood, e.g. CDe/cde genotype.
- Volume of fetal blood entering into the maternal circulation (0.1 mL is considered as critical sensitizing volume).
MECHANISM OF ANTIBODY FORMATION IN THE MOTHER:
If the ABO compatible (mother and fetus have the same ABO group or when the fetus is group “O”), Rh-positive fetal red cells enter the mother’s blood, they remain in the circulation for their remaining lifespan. Thereafter, they are removed from the circulation by the reticuloendothelial tissues and are broken down with liberation of the antigen.
The antibody production is related not only to the responsiveness of the reticuloendothelial system but also to the amount of Rh antigen liberated, therefore to the number of red cells that have entered the
maternal blood. Because this takes a long time, immunization in a first pregnancy is unlikely. Detectable antibodies usually develop after 6 months following larger volume of fetomaternal bleed. But, if the
fetomaternal bleed is less than 0.1 mL, the antibody may not be detected until boosted by further Rh
stimulus. Antibodies once formed remain throughout life.
TYPES OF ANTIBODIES - Two types of antibodies are formed:
1) IgM-this type of antibody is the first to appear in the maternal circulation and agglutinates red
cells containing D when suspended in saline. IgM being larger molecules cannot pass through the
placental barrier and is not harmful to the fetus.
2) IgG-it is also called incomplete or blocking antibody. It will agglutinate the red cells containing D only when suspended in 20% albumin. Because of its small molecule, it can cross the placental barrier and cause damage to the fetus. It appears at a later period than does the IgM antibody. It is important
to recognize the preponderance of one or the other type of antibody than the actual level of the titer.
HOMOEOPATHIC MEDICINES FOR MANAGING ALLOIMUNISATION: -
1) Cal Phos: - this remedy can help to strengthen a woman who tends toward easy tiredness,poor digestion, cold hands and feet, and poor absorption of nutrients. A person who needs cal phos is often irritable because of tiredness, and may long for a travel or a change of circumstances.
2) Caulophyllum: - this remedy may be helpful in women with weak muscle tone in the uterus. A history of irregular periods, slow and difficult labour with previous deliveries, or weakness of the cervix may bring this remedy to mind. She typically feels nervous, shaky, and trembling.
3) Carbo Veg: - this remedy can be helpful to a woman who feels weak and faints during pregnancy, with poor circulation, a general feeling of coldness, and a craving for fresh or moving air. She may also have frequent digestive upsets with burning pain and a tendency to belch.
4) Actaea racemosa: - this remedy can be helpful to women who are nervous and talkative, with a tendency to feel fearful and gloomy during pregnancy. They may become overagitated and a dear of miscarriage prevails.
5) Ferrum phos: - this remedy can be helpful for nervous sensitive women who feel weak or tired with easy flushing of face and a tendency towards anaemia. A woman who needs this remedy often has a slender build and may develop frequent neck and shoulder stiffness
ABHI HOMEO HALL is a one and half decade old renowned clinic that offers the best quality, non-toxic and highly effective treatment in Ranchi, Patna and Delhi.
Read More
